Torus mandibularis is a benign bony growth that develops on the lingual (inner) surface of the mandible, most commonly in the premolar region. Although it is a well-recognized anatomical variation in dentistry, it is frequently overlooked by patients and sometimes even underestimated in its clinical significance. For most individuals, torus mandibularis is an incidental finding during routine dental examination, requiring no treatment. However, in certain clinical situations, it can influence oral hygiene, planning for denture and patient-comfort.
Clinical Appearance
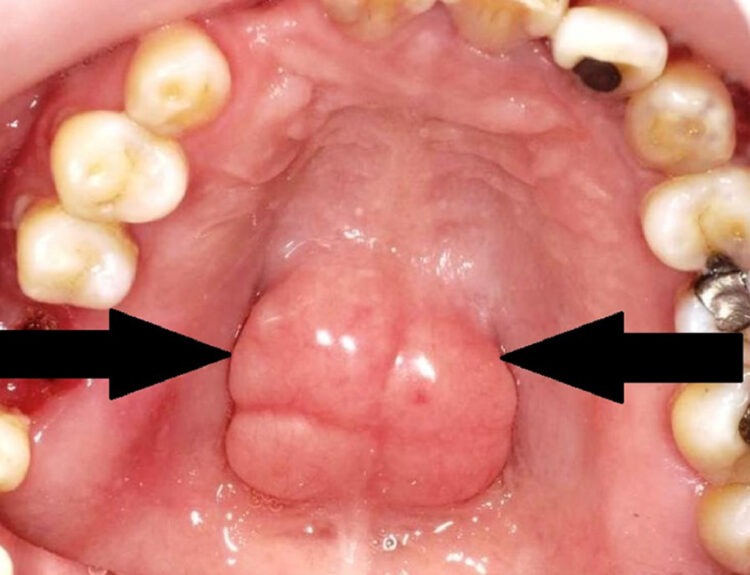
Torus mandibularis is an outgrowth of dense outer layer of jaw bone. It typically presents as a bilateral, symmetrical, nodular or smooth bony bulge on the inner aspect of the lower jaw. The overlying mucosa is thin and stretched and has poor blood supply, making it susceptible to trauma. The size of the torus can range from small, barely noticeable elevations to large, lobulated masses that occupy a significant portion of space between the tongue and lower jaw (lingual sulcus). The condition usually becomes evident in early adulthood and tends to grow slowly over the period of time. It rarely appears in childhood and generally stabilizes after middle age.
Etiology
The exact cause of torus mandibularis remains unclear and dentists consider it as a multifactorial condition. Genetic predisposition plays a significant role, as researchers report higher prevalence within families and certain ethnic groups. Environmental and functional factors also play a role to contribute.
Researchers freqyently consider occlusal stress and parafunctional habits such as bruxism and teeth clenching as its contributing factors. The mandible responds to excessive masticatory forces by reinforcing bone in areas of stress, leading to bulge formation. Dietary factors, particularly a diet rich in calcium and vitamin D, are also contributing factors, though evidence remains inconclusive.
Epidemiology
The prevalence of torus mandibularis varies widely among populations, ranging from 5% to over 40% in different studies. It is more commonly reported in adults than in children and appears slightly more frequently in males than females. Certain populations in Asia and Northern Europe show higher prevalence, supporting the role of genetic factors.
Clinical Significance
In most cases, torus mandibularis is asymptomatic and requires no intervention. Many patients are unaware of its presence until informed by a dentist. However, its clinical significance increases under specific circumstances.
Oral hygiene can be challenging in patients with large torus, as plaque and calculus may accumulate in the adjacent areas due to limited access for brushing and flossing. This may predispose to localized gingival inflammation.
A torus mandibularis can pose difficulties in the fabrication of removable partial or complete dentures. The thin mucosa overlying the torus is prone to ulceration under denture pressure. In such cases, denture design modifications or surgical removal of the torus may be necessary.
It rarely affect speech and mastication, but very large torus may interfere with tongue movement, causing discomfort or altered speech in extreme cases.
Diagnosis
Diagnosis of torus mandibularis is primarily clinical. On palpation, it feels hard, non-compressible and continuous with the underlying bone. Radiographically, it appears as a radiopaque mass superimposed over the roots of the mandibular teeth, although imaging is not routinely required unless the diagnosis is uncertain.
Differential diagnosis includes benign and malignant bone tumors, osteomas and other hard swellings. The bilateral and symmetrical nature, slow growth and lack of symptoms usually distinguish torus mandibularis from pathological conditions.
Management and Treatment
No treatment is indicated for torus mandibularis unless it causes functional problems or interferes with dental procedures. Patient reassurance and education are sufficient. Emphasis should be placed on maintaining good oral hygiene and avoiding trauma to the area. Clinicians recommend its surgical removal is in selected cases, such as:
- Interference with denture construction
- Recurrent ulceration of the overlying mucosa
- Difficulty in speech or mastication
- Use of the bone as an autogenous graft source in gumor implant surgery
Dentists oerform surgical excision usually under local anesthesia and involves careful flap design due to the thin mucosa. Healing is generally uneventful, although postoperative discomfort and edema may occur.
Its awareness among dental clinicians and patients alike ensures appropriate diagnosis, reassurance and management. Recognizing torus mandibularis as a variation of normal anatomy rather than a pathological entity helps prevent over treatment and alleviates patient concern, reinforcing the importance of careful clinical examination in routine dental practice.
Read our full disclaimer.